
Clinical Exercise: Liver Resection
Scenario:
A patient with a history of hepatitis presents with a localized carcinoma on the superficial right lobe spanning hepatic segments 4a and 8 detected by MRI. The mass is approximately 4cm in diameter and no indications of any metastatic masses elsewhere .
Diagnosis:
The MRI indicates that the mass is a hepatocellular carcinoma, the most common type of primary liver carcinoma. Typically, a biopsy is not required for this type of tumor as the MRI characteristics are sufficient for high confidence determination. Due to the risk of bleeding or seeding (spread of individual cancer cells to other locations when disrupted during a biopsy) you decide against performing a biopsy.
You recognize that a well defined mass with no indications of metastatic spread is a candidate for an anatomic resection of the affected hepatic segments.
Mechanism:
Liver resection takes advantage of the anatomic segmental organization of the liver. Hepatic segments each have a discrete vascular pedicle in the portal triad (the pedicles carry a branch of the left or right hepatic arteries, portal vein, and bile ducts). Each segment is defined by the hepatic veins draining back from the liver segments to the inferior vena cava. The hepatic veins travel to the periphery of the segment while the vascular portal triad pedicles are more centrally located (similar to how in the lung pulmonary veins are to the periphery of bronchopulmonary segments).
Resection of liver segments can occur without compromising the vascular supply or drainage of surrounding segments, allowing removal of regions of the liver safely. This can be for removing a carcinoma or for removing a lobe for liver transplants.
Treatment (perform these steps on the donor in a mock procedure):
1) Arrange the gastrointestinal block organs on the dissection train in approximately the orientation they would be in the body.
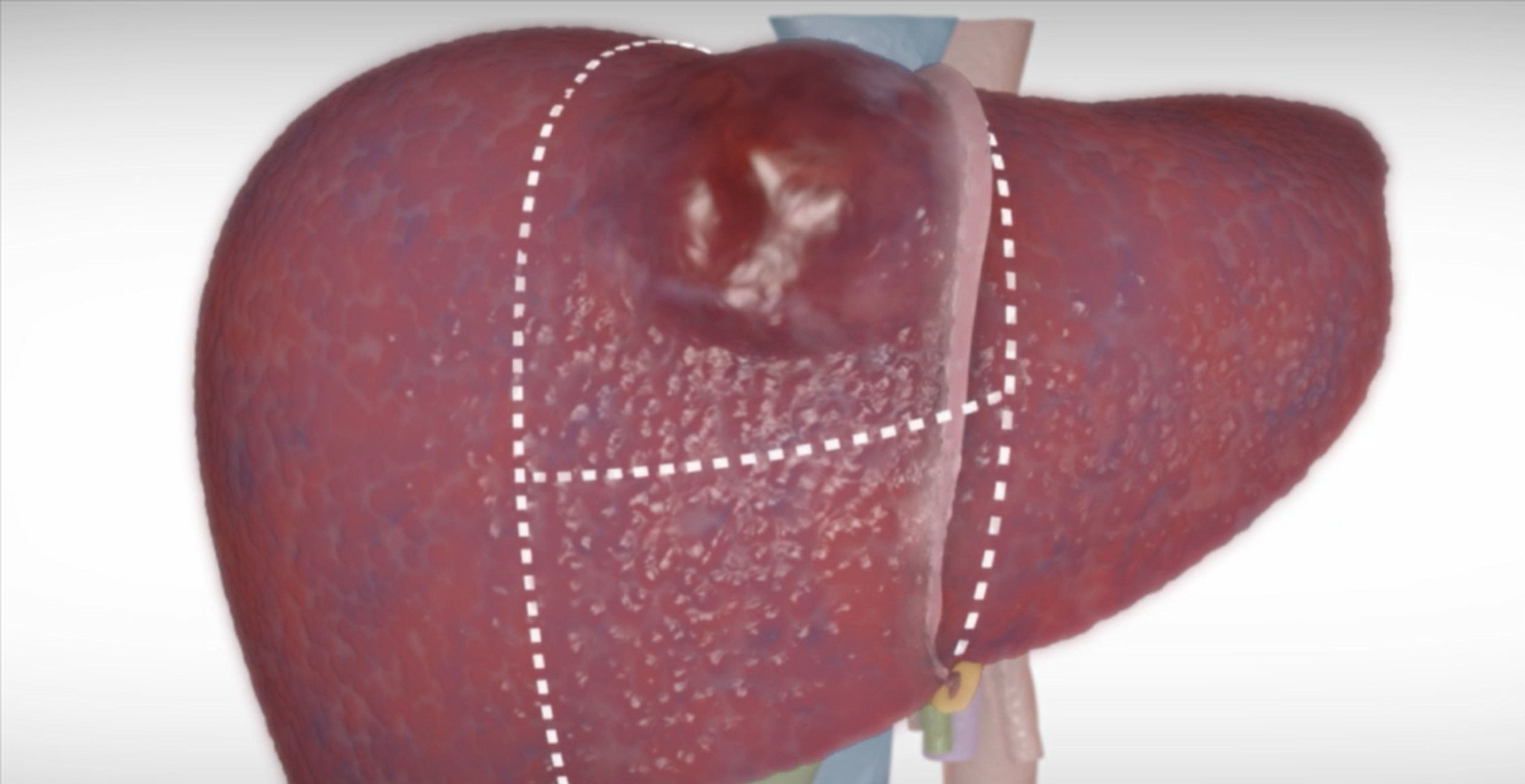
2) Using a surgical marker, draw three pre-surgical incision lines on the anterosuperior surface of the liver.
A key component of resection is to ensure there is 1cm of healthy tissue margin removed along with the mass. That ensures complete removal of the mass and eliminates the risk of seeding cancerous cells by inadvertently cutting through the cancerous tissue with a scalpel.
a) a line from the inferior vena cava following just to the left of the falciform ligament 1cm to the left of the imaginary mass.
b) a line from the inferior vena cava 1cm to the right of the imaginary mass (about a third of the way across the right lobe)
c) a horizontal line linking the other marks approximately 1cm inferior to the imaginary mass
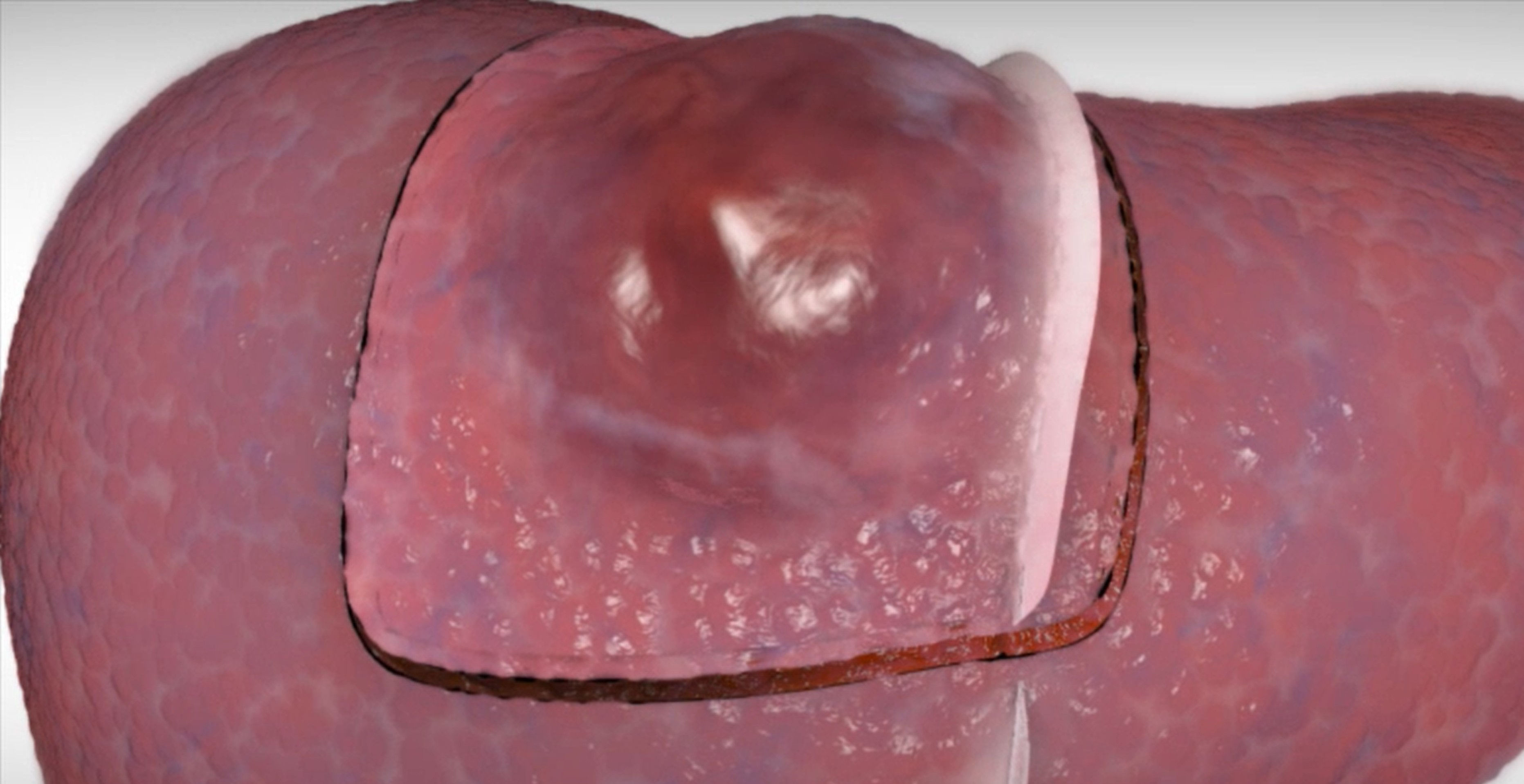
3) Using a scalpel make an approximately 1-2cm deep incision following the surgical planning lines.
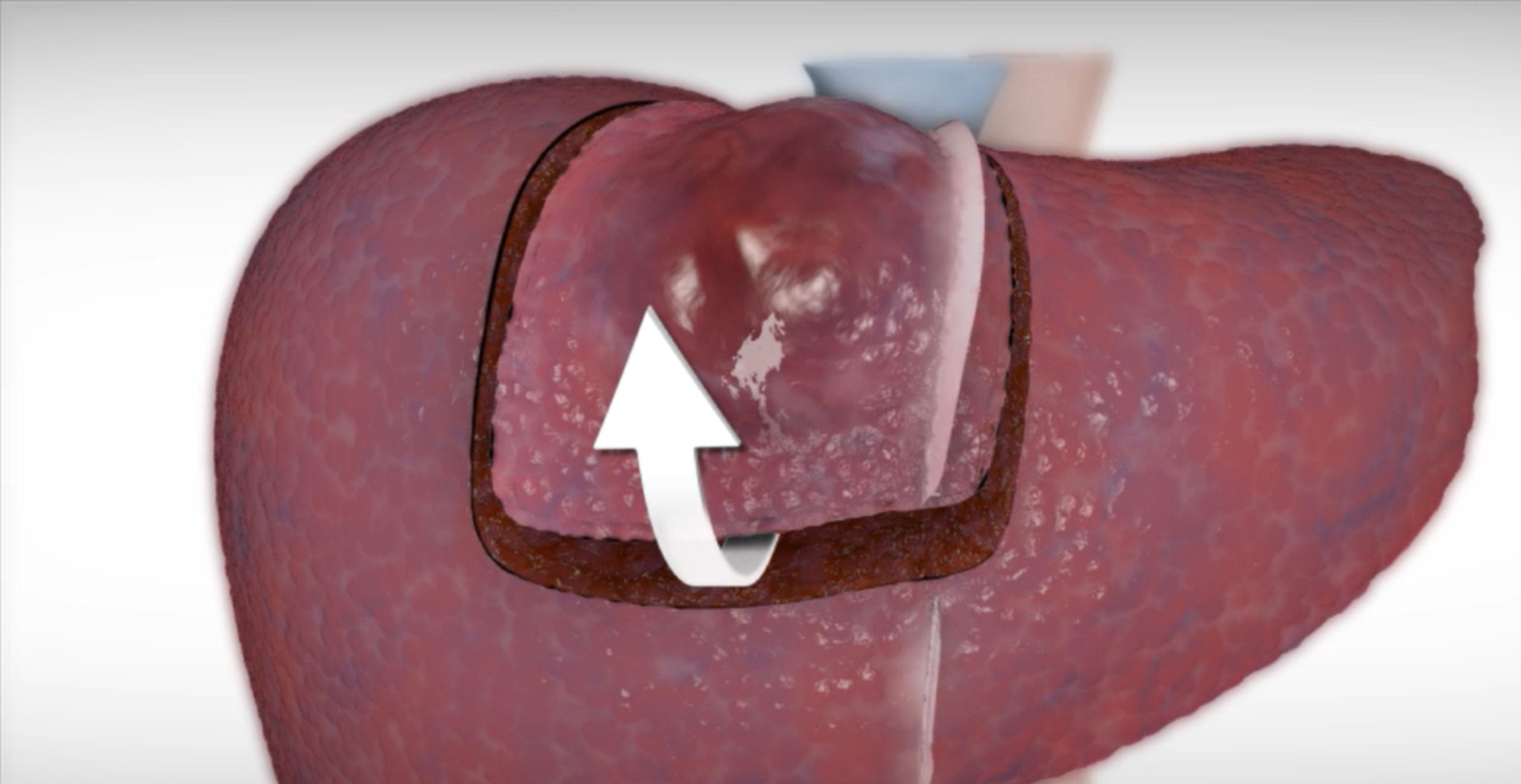
4. Have one member of the team use a scalpel handle (no blade) to 'lever' the hepatic segment while another member of the teem continues to deepen and extend the cut aiming at the middle hepatic artery origin from the inferior vena cava.
In cases the liver density may be such that levering the segment is not readily achievable, in this case use the 6" large knife in the tool tray below the table to deepen the lateral incisions and potentially use the large knife to cut the deep lines for excising the segment.
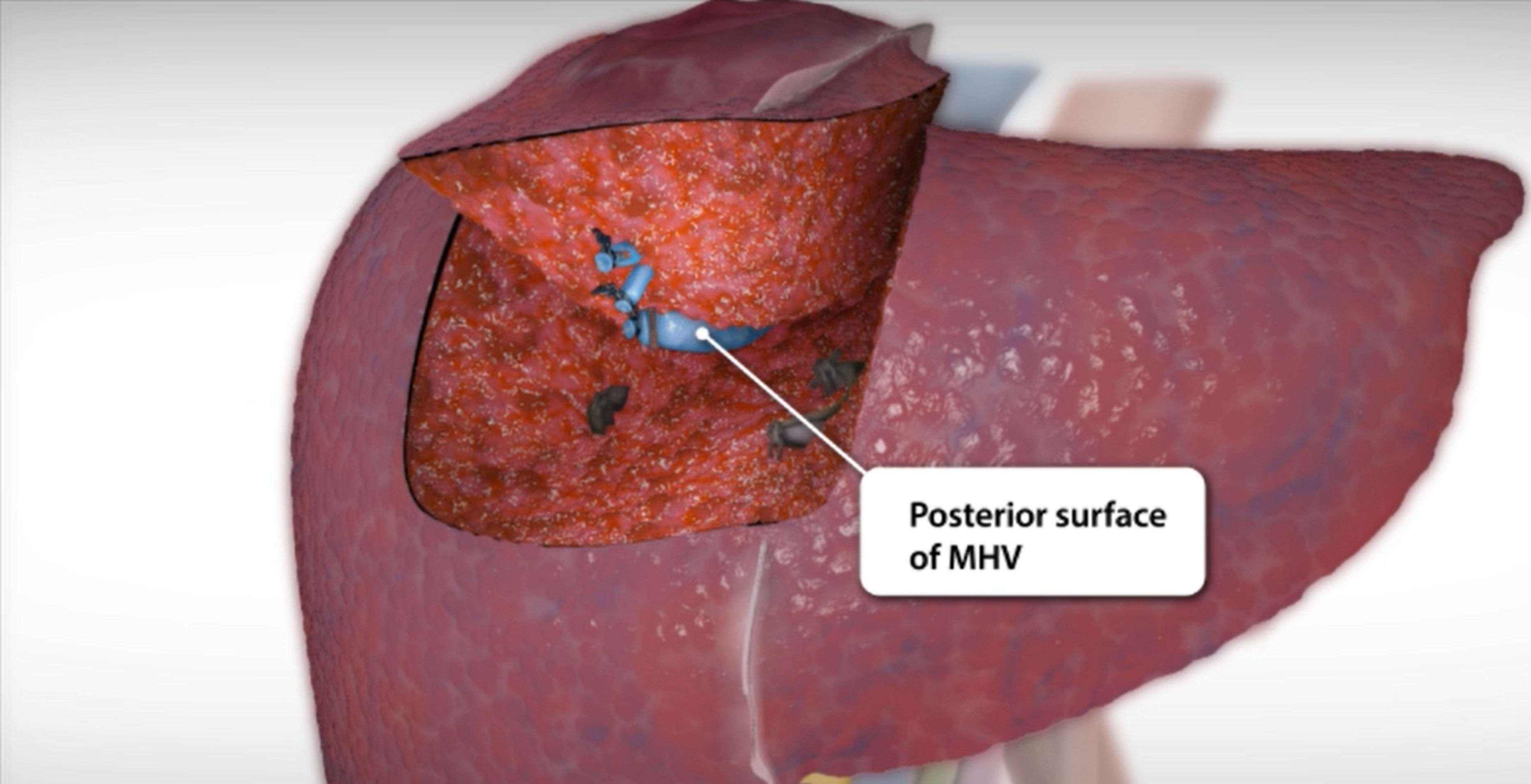
5. Depending on the exact angle of the incision, as you continue to lever out the wedge of liver tissue you may observe the inferior surface of the middle hepatic vein, which defines the boundary between the 4a and adjacent 8 hepatic segments.
In addition you will see other veins and portal triad pedicles for the segment sliced through by your scalpel cuts. In the living, each of these would be isolated and ligated during the procedure.
6. Completely remove (resect) the liver wedge by transecting the base of the segment including the middle hepatic artery at the origin with the inferior venal cava.
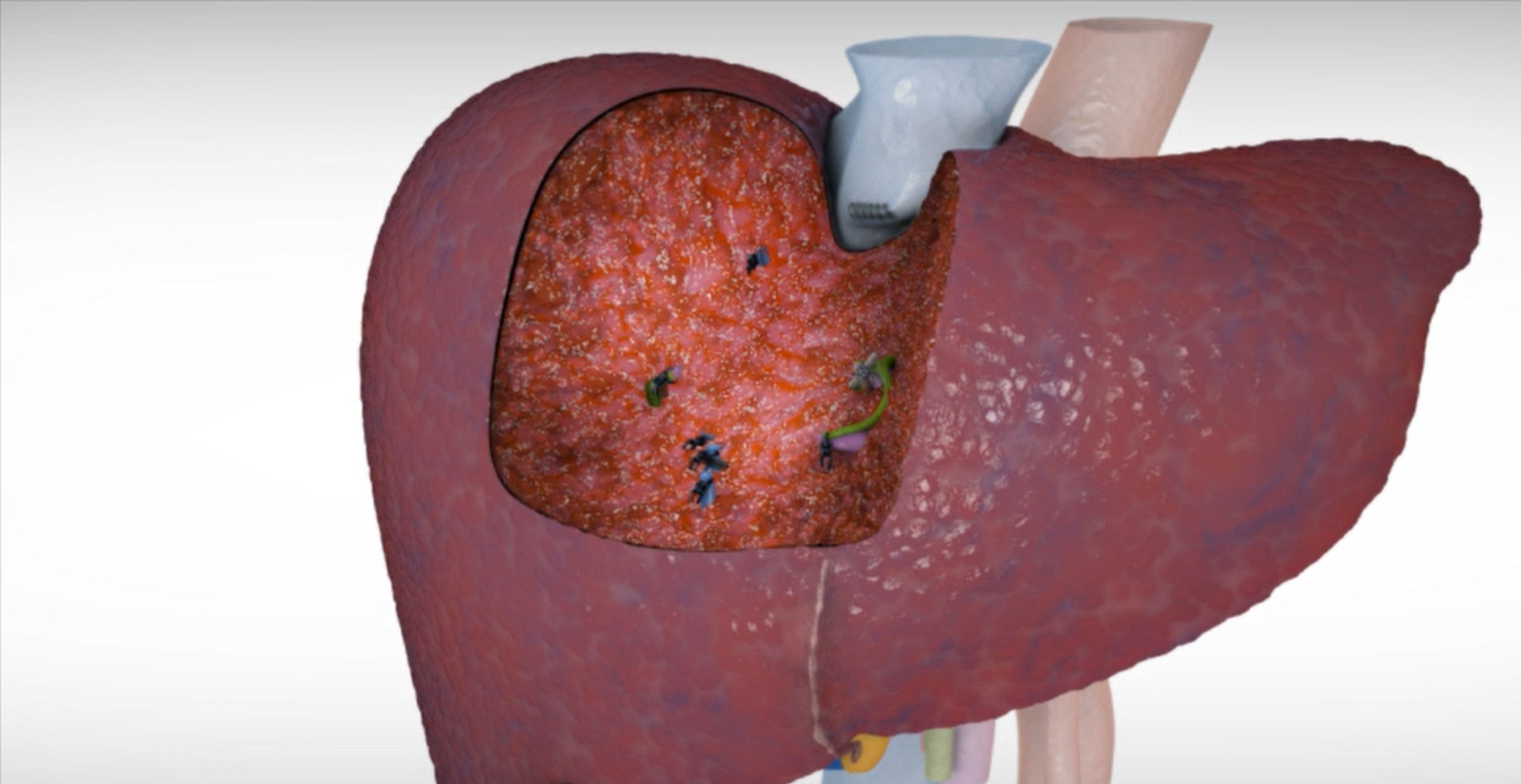
Observe how the exposed surface of the liver is solid tissue interspersed with cut branches of hepatic veins and portal triad vessels. In the living, the larger vessels are ligated and smaller vessels sealed by electrocautery.
Outcome:
The liver resection is a success with histopathology evaluation confirming clean margins removed around the hepatocellular carcinoma.
Liver regeneration occurs rapidly after resection of liver tissue through a complex feedback loop regulating absolute liver mass proportional to total body mass. The patient exhibits a normal recovery of liver mass, with their liver mass restored after approximately 2-4 weeks.