Clinical Exercise: Thumb carpometacarpal Platelet Rich Plasma Injection
Scenario:
You are caring for a patient with progressive thumb carpometacarpal osteoarthritis (TCMC-OA) who is a concert pianist. Conservative management through activity modulation has become of limited use in diminishing the patients discomfort whenever moving their thumb. The patient reports frequent base of thumb pain and functional impairment when using their thumb as a consequence.
Diagnosis:
Thumb carpometacarpal osteoarthritis is a progressive disabling/debilitating condition that results in base of thumb pain and impaired function of the hand manifesting as reduced range of motion and grip/pinch strength.
You make the determination to try a regenerative medicine approach with platelet rich plasma injection into the carpometacarpal joint.
Mechanism:
Osteoarthritis is a progressive loss of the articular
cartilage covering the bone surfaces within the joint. This articular cartilage
is essential for providing a low friction surface for movement. While the
cartilage itself has no nerve innervation, the underlying bone is richly
innervated such that when the bone is exposed by loss of cartilage,
considerable pain is elicited with movement or chronically even without movement
through ongoing joint inflammation.
Platelet-rich plasma (PRP) is produced from the patient’s blood by centrifugal separation of the platelet fraction. This concentration of platelets in plasma is injected into a joint or other target (e.g. ligaments, tendons, etc.). Platelets have been shown to release growth and inflammatory factors that stimulate reparative cells. They are thought to function as a type of regenerative medicine to harness endogenous factor production from the cells to stimulate damaged tissue healing. Their use has been linked to improved symptoms, reduced need for opioids and reduced over-the-counter use of non-steroidal anti-inflammatory medications (NSAIDs). Indeed, anti-inflammatory drug use should be discontinued at the time of PRP treatment as those drugs may suppress some of the inflammatory factor platelet secretions necessary for the cellular regenerative functions.
Treatment (perform these steps on the donor in a mock-procedure):
To treat this patient, you need to inject PRP into the
thumb carpometacarpal joint space
PREPARATION: Send a member of your team to the instrument
supply tables to fetch a 25-gauge needle, a 3ml syringe, and one of the purple
surgical skin markers.
Fill the syringe with several milliliters of wetting agent
(simulating the PLP fluid).
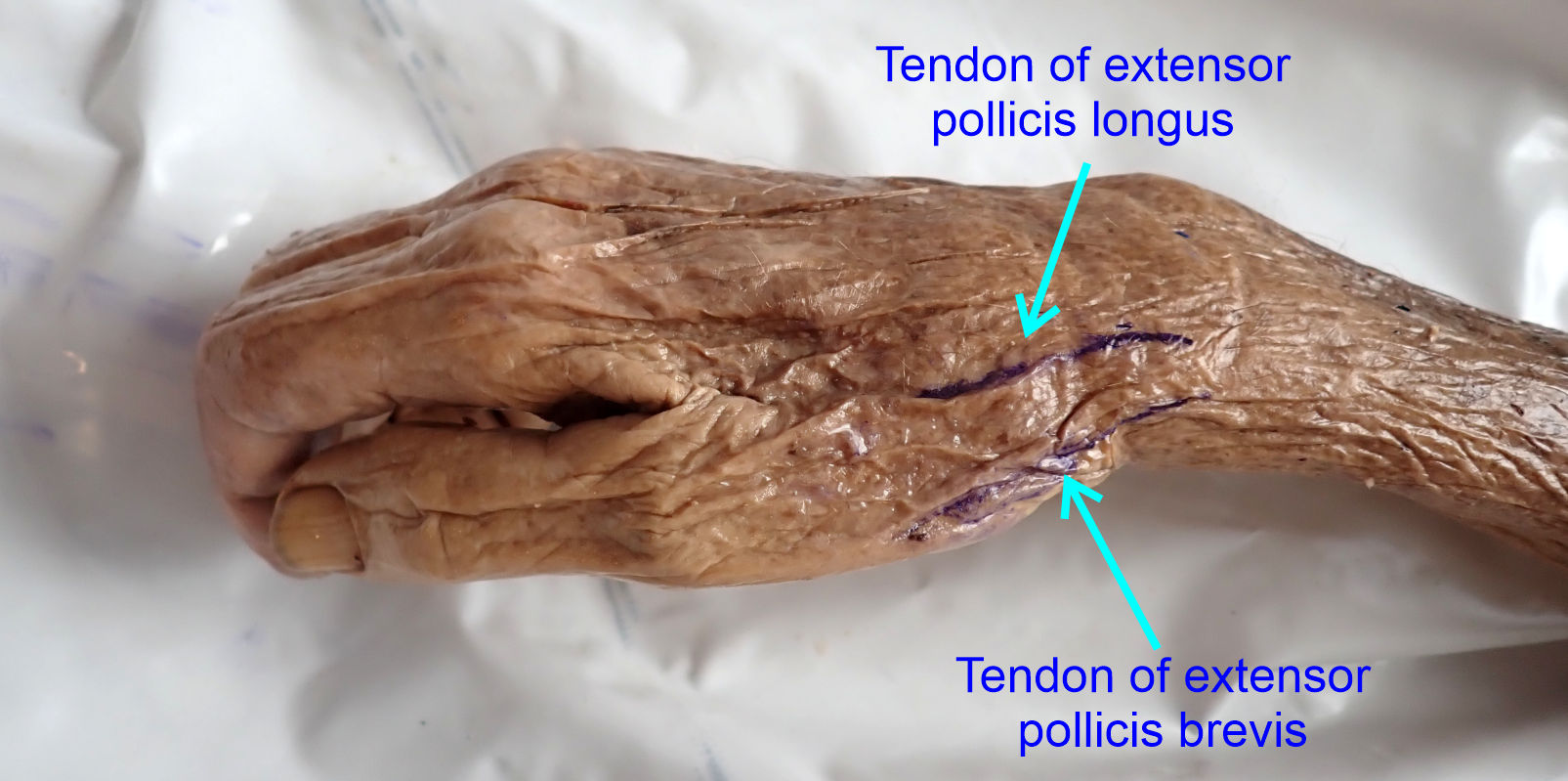
1) Palpate for the 'anatomic snuffbox' which is the
triangular region between the tendons of the extensor pollicis brevis and
abductor pollicis longus.
2) Mark the trajectory of the tendons with one of the
surgical skin markers.
The thumb carpometacarpal joint (i.e. base of thumb) is approximately at the proximal third of the snuffbox and may be palpable on your donor by moving the thumb about.
It will be easier to palpate on a living patient and you can
palpate upon yourself or a willing partner while moving the thumb to explore the
anatomic snuffbox anatomy.
Typically, the region would be injected with a local
anesthetic for patient comfort, a step we will skip with our donors.
3) Place the needle at 90 degrees to the skin surface just
dorsal to the tendon of the extensor pollicis brevis and insert the needle aimed
at the approximate location of the thumb carpometacarpal joint (or slightly
proximal).
If you impact against bone change the angle to 'walk' the
needle trajectory more distal or proximal till you find the joint space.
When entering the joint, you may feel a slight 'pop'
sensation as the needle penetrates the joint capsule.
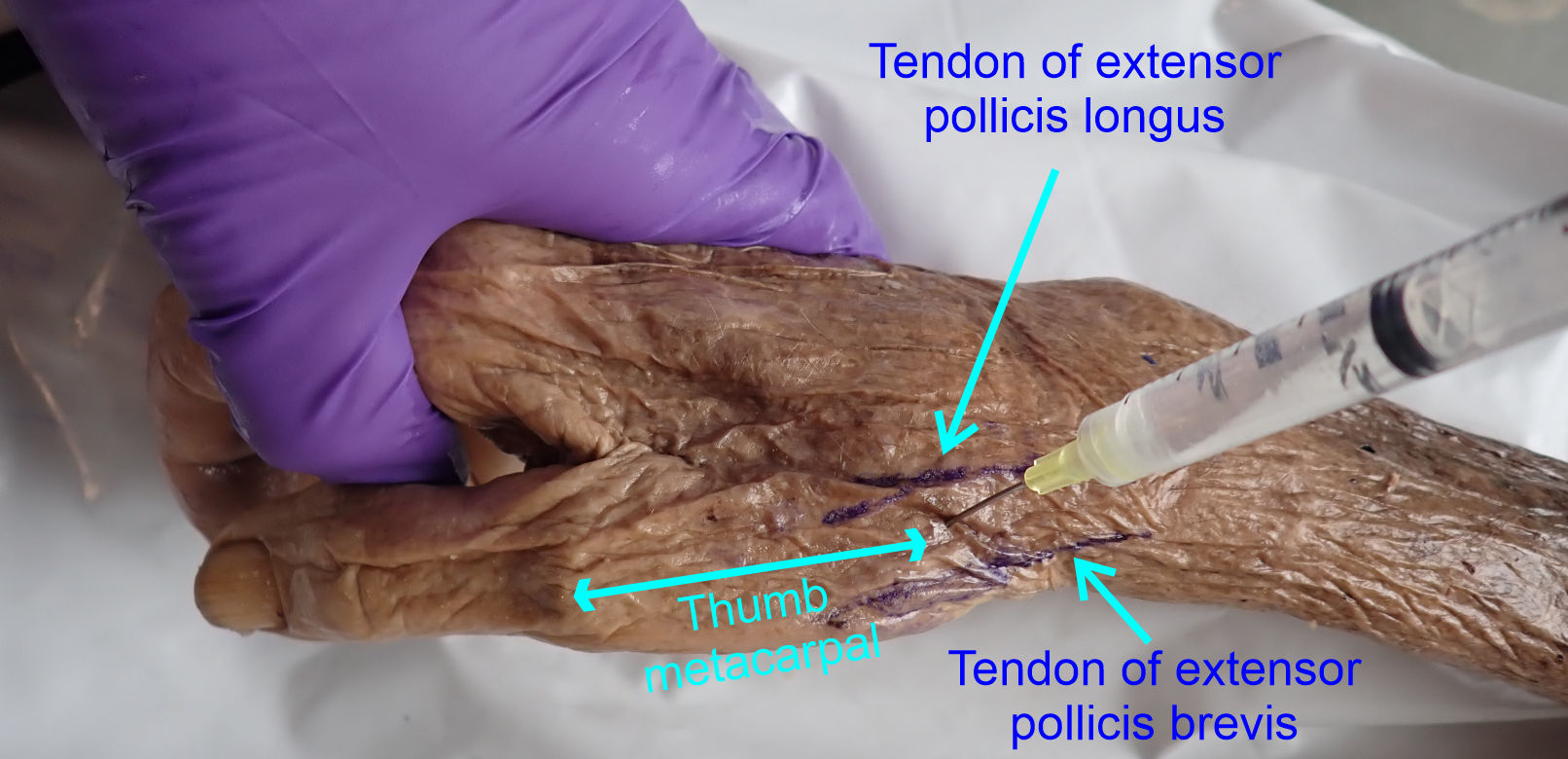
4) Inject approximately 0.5ml of fluid into the joint
space.
Injecting too much volume into the joint space can increase
pressure inside the capsule and yield some acute pain when the local anesthetic
wears off.
NOTE: when finished the procedure ensure that the syringe and attached needle
are collected in one of your trays and transported to the sharps containers for
disposal.
Do not attempt to re-cap a needle - Re-capping is a leading
cause of needle-stick injury.
Never transport needles by hand - Always transport entire
syringe/needles in a tray.
Outcome:
A dressing is placed over the injection site and the patient is sent home to recover. Functional outcome was excellent with daily living activities recovering within the month. At 12 months follow-up, no recurrences or complications were identified. The patient’s self-reported satisfaction was high and they were able to return to routine piano activity with few limitations.