PROCEDURE
1.
PRE-WORK
(before lab) review the organization of the
anterior bones of the neck from your atlas or on an articulated skeleton in the lab.
(Netter022)
(Netter024)
Mandible - Examine the mandible and identify the mentum at the most anterior point on the mandible inferior to the teeth. The body of the mandible extends laterally and posteriorly to each side forming a horseshoe-like shape holding the teeth.
Hyoid bone - This bone is a C shaped bone located inferior to the mandible and posterior to the tip of the chin (the mental protuberance).
Unlike most bones, the hyoid bone has no joints and is only distantly articulated to other structures by muscle/ligament connections serving as an important fulcrum on which the muscles can act.
Clavicle: The clavicle extends from the superolateral aspect of the sternum (sternal end of the clavicle) lateral out to the acromion forming the lateral shoulder. Structures immediately deep to the clavicle form part of the root of the neck.
Radiology - X-ray films of the neck can be useful to identify skull and vertebral features, but are of limited use for the various soft tissue and fascial regions. The hyoid bone is quite thin and visible as a small bony feature just inferior to the mandible. The lucent (dark) area of the pharynx, the larynx and continuation anteriorly of the trachea airspace is readily apparent on a lateral film. The esophagus is closed/collapsed when not swallowing so this cannot be distinguished in the soft tissue posterior to the trachea. (Rad7001)
2. PRE-WORK (before lab) the
organization of the
fascia of the neck from your atlas.
(Figure779)
(Netter033)
Cervical fascia - The entire neck is sheathed by a cervical fascia formed by dense investing fascia that splits and recombines to surround the trapezius and sternocleidomastoid muscles (see in previous dissections).
Prevertebral fascia - The vertebral column and associated muscles are surrounded by a sheath of prevertebral fascia.
Carotid sheath - The vascular elements on each side of the neck are surrounded by a more delicate carotid sheath.
Pretracheal fascia - The trachea, esophagus and associated elements are cased by a thin pretracheal fascia.
These layers within the neck define a series of compartments which bacterial infection may spread within or between.
Superficial fascia - The superficial fascia lies superficially to the sheath of cervical fascia. Within the superficial fascia is the platysma muscle sheet which functions to tighten the skin of the neck. Also within the superficial fascia are a network of veins including the large external jugular vein running superior to inferior anterolateral on the neck.
3. PRE-WORK
(before lab) the triangles of the neck.
(Figure746) (Netter036)
Anterior Triangle - The anterior triangle of the neck is bounded by the anterior border of the sternocleidomastoid muscle, the jugular notch, and the lower border of the mandible.
The anterior triangle is subdivided into regions useful for conceptual organization.
Suprahyoid Region - The suprahyoid region is everything between the hyoid bone inferiorly and the mandible superiorly. This region has multiple muscles and other structures forming the floor of the mouth (we will examine these in later courses).
Infrahyoid Region - Everything inferior to the hyoid bone, medial to the sternocleidomastoid muscle and superior to the jugular notch and clavicle.
The infrahyoid region is often further subdivided.
Muscular Triangle (infrahyoid) - This region is bounded by the hyoid bone, the anterior margin of the sternocleidomastoid muscle, the superior belly of the omohyoid muscle, and the jugular notch.
Carotid Triangle (infrahyoid) - The carotid triangle is bounded by the stylohyoid muscle superiorly, the sternocleidomastoid muscle posteriorly, and the superior belly of the omohyoid inferiorly.
The carotid triangle is where you can readily feel a carotid pulse. Pressing 2 fingers into the region just medial to the sternocleidomastoid muscle at or just superior to the level thyroid cartilage to feel your own carotid pulse.
4. Before cutting into the skin of the
anterior neck, identify several bony landmarks by palpation:
(Netter022)
a) The jugular notch (part of this was excised during an earlier lab) and the sternoclavicular joint.
b) Moving superiorly from the jugular notch, feel along the tracheal rings to the cricoid cartilage. Immediately superior is the thyroid cartilage, together forming the larynx.
c) Superior to the thyroid cartilage is the horseshoe shaped hyoid bone, which is located inferior to the mandible and posterior to the mental protuberance.
CLINICAL EXERCISE - Cricothyrotomy
5. Airway management and breathing are clearly the most important considerations in any trauma or emergency medical situation. Most of the time this is achieved by ventilation (either by mouth-to-mouth or with a ventilation mask/bag) or intubation (insertion of a tube into the upper airway followed by ventilation). However, in cases where these approaches are not possible, a temporary alternate airway can be established by incising a hole through the front of the airway in the neck.
In this clinical exercise, you have the chance to perform a cricothyrotomy to your donor in a mock surgical intervention.
For the steps to
take:
------
click here ------
6. Lift the donor slightly and place the wood
support block longitudinally directly under the middle of the back.
(Figure237)
The wood support blocks are on the foot of the shelf under your table. At the end of a lab using blocks they should be returned to this location.
This causes the shoulders to sag posteriorly and open the gap in the manubrium at the jugular notch, giving improved access to the superior mediastinum.
7. Extend the cricothyrotomy skin incision inferiorly to
the jugular notch, such that the skin at the midline is completely separated.
(Figure747a) (Photo7100)
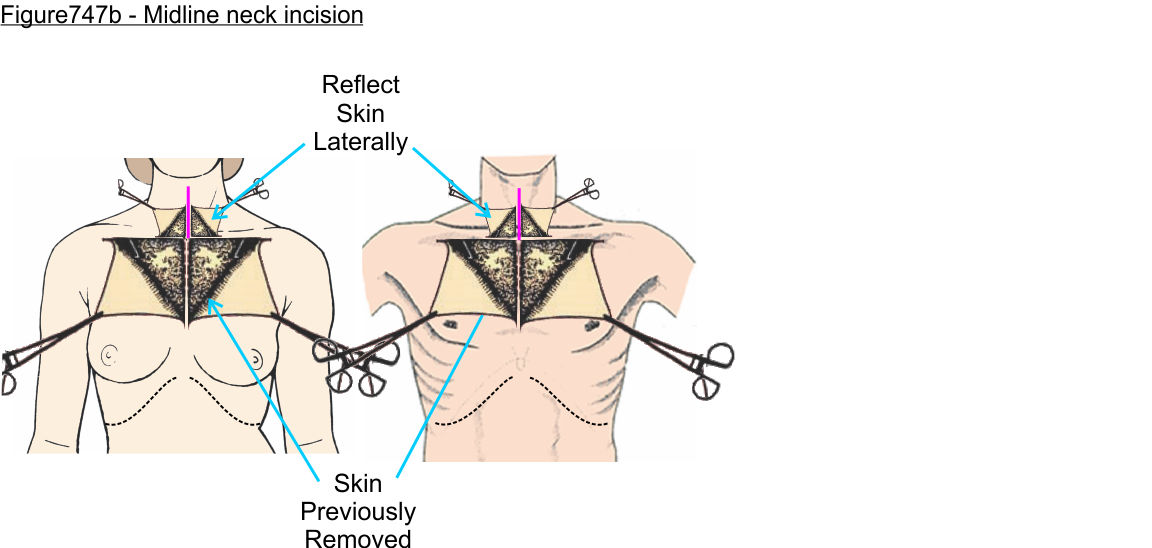
8. Working laterally reflect the skin and superficial
fascia containing fibers of the platysma muscle.
(Figure747b) (Photo7101)
You may find it helpful to position the wood block horizontal under the shoulders such that the donor head tilts posteriorly better exposing the neck.
The platysma muscle is one of the muscles of facial expression and consists of a thin sheet of muscle fibers oriented superior to inferior 'draping' from the mandible down to the clavicle.
The muscle functions to tighten/wrinkle the skin of the neck during speech or head/neck movement. This muscle frequently becomes less distinct with age, contributing to the looser skin tone of elderly individuals. Thus, in our donors there may only be residual fibers present in the subcutaneous tissue.
9. Extend the midline incision to just superior to the
level of the hyoid bone (approximately 1-2" from the chin) and
reflect skin widely to expose the sternocleidomastoid muscle.
(Figure747b) (Photo7102)
The anterior triangle of the neck is bounded by the anterior border of the sternocleidomastoid muscles and the ramus of the mandible.
The carotid and muscular triangles are subdivisions of the anterior triangle inferior to the hyoid bone.
The muscular triangle is bounded by the hyoid bone, the anterior margin of the sternocleidomastoid muscle, the superior belly of the omohyoid muscle, and jugular notch.
PROCEDURE - Muscular Triangle
10. Separate the deep/investing fascia at the anterior and
lateral borders of the sternocleidomastoid muscle such that a blunt probe or
instrument can pass deep to the muscle.
(Figure748)
(Netter032) (Photo7103)
The investing layer of fascia completely encircles the neck with the sternocleidomastoid muscle anteriorly and the trapezius muscle posteriorly embedded inside the fascia. The fascia splits to pass over the superficial and deep surfaces of these muscles.
The sternocleidomastoid and trapezius muscles are both innervated by the accessory (CN11) nerve.
11. Using the blunt probe or instrument as a guide transect
the sternocleidomastoid muscle as close to the bone of the clavicle and
manubrium as possible.
(Figure748)
(Netter032) (Photo7104)
The sternocleidomastoid muscle derives the name from the inferior two heads that attach to the manubrium of the sternum and the clavicle as well as the superior attachment to the mastoid process of the skull.
12. Reflect the sternocleidomastoid muscle superolateral
using blunt dissection to separate the muscle from the underlying structures.
(Netter032) (Photo7105)
(Photo7106)
As you bluntly separate the sternocleidomastoid muscle it is common for the superior belly of the omohyoid muscle to lift at the same time.
Watch for this muscle belly and as needed use blunt dissection to separate along the fascial plane between the superior belly of the omohyoid and sternocleidomastoid muscles so you can freely reflect the sternocleidomastoid muscle.
13. With the sternocleidomastoid muscles reflected
superolateral, separate the superior belly of the omohyoid muscle from the
surrounding fascia.
(Figure749a) (Netter035)
(Photo7107)
Observe that the muscle belly becomes pale and more cord-like as it makes a lateral turn towards the shoulder. The paler tissue is the intermediate tendon separating the superior belly of the omohyoid muscle from the inferior belly of the omohyoid muscle.
Thus, the omohyoid muscle consists of two muscle bellies (superior and inferior) connected by a tendinous region.
The fascial sling that 'hocks' the intermediate tendon of the omohyoid muscle, forming acute angle between the two bellies of the muscle, is integrated into the deep surface of the investing fascia. Thus, causing the lifting of the omohyoid muscle during reflection of the sternocleidomastoid muscle in the steps above. This arrangement also means that the sling is not observable as a distinct structure.
14. Dissect into the fascia immediately lateral to midline of the neck
to isolate and separate the sternohyoid
muscle from the fascia.
(Figure749a) (Netter032) (Netter035)
(Photo7108)
The sternohyoid muscle, as the name implies, connects inferiorly with the sternum and superiorly with the hyoid bone. The muscle functions to depresses the hyoid bone during swallowing.
If you gently place your fingers on the lateral sides of your own hyoid bone and swallow, you will feel the bone 'jump' superiorly and then be depressed back to the normal position.
This muscle is part of a group of muscles collectively called the strap muscles (or infrahyoid muscles) which are all long and flat, resembling straps.
The group of strap muscles includes the sternohyoid, sternothyroid, thyrohyoid, and omohyoid muscles, which all derive their names from their attachments.
15. Free the sternohyoid and omohyoid muscles completely
from any underlying fascia.
(Figure749a) (Netter032) (Netter035)
(Photo7109)
16. Retract the omohyoid and sternohyoid muscles laterally
and expose the sternothyroid muscle.
(Figure750a) (Netter035)
(Photo7110)
The sternothyroid muscle is immediately deep to the inferior half of the sternohyoid muscle. As the name implies, the sternothyroid muscle attaches to the sternum and thyroid cartilage of the larynx. When contracted, it depresses the larynx.
17. Dissect along the medial edge of the sternothyroid
muscle and reflect the muscle sufficiently laterally to expose the underlying thyroid gland.
(Figure750a) (Netter087)
(Photo7111)
The thyroid gland is covered by the more superficially located strap muscles (sternothyroid and thyrohyoid). The gland has left and right lobes that are linked by an extension of glandular tissue crossing the trachea inferior to the cricoid cartilage, called the isthmus of the thyroid.
Blood vessels enter the superior side of the thyroid gland (the superior thyroid artery and vein) and the inferior side of the gland (the inferior thyroid artery and vein).
In approximately 25% of individuals there is also an extension of glandular tissue running superiorly up to the level of the cricoid or thyroid cartilage. If present, this is called a pyramidal lobe.
18. Dissect superior to the thyroid cartilage in line with
the sternothyroid muscle to find isolate the thyrohyoid muscle.
(Figure750a) (Netter035)
(Photo7112)
The thyrohyoid muscle spans from the thyroid cartilage to the hyoid bone.
Functionally if the hyoid bone is 'locked' in position by other muscles the thyrohyoid pulls the thyroid cartilage towards the hyoid bone. Alternatively, if the hyoid bone is non-fixed then the muscle can pull the hyoid towards the thyroid cartilage.
PROCEDURE - Carotid Triangle
19. Remove fascia from the anterior surface of the trachea
inferior to the thyroid gland and observe the brachiocephalic trunk crossing
from the vessel origin on the arch of the aorta over to the right side of the
trachea.
(Netter087)
(Netter199)
(Photo7113)
Tracheal rings - The trachea has a series of C shape cartilage rings that face anteriorly (i.e. the open side of the C is pointed posteriorly). Palpate along the anterior surface of the trachea you can feel the ridges of the cartilage presenting similar to a corrugated hose arrangement.
Cricoid cartilage - Moving superior is the cricoid cartilage. This is a signet-ring shaped cartilage with a slight anterior arch/bulge.
Thyroid cartilage - Just above the cricoid cartilage is the thyroid cartilage. At the anterior midline the thyroid cartilage forms a distinct bump, the laryngeal prominence (or Adam's apple). Sliding your fingers to each side of the thyroid prominence you can feel the posteriorly directed laminae (plates of cartilage).
20. Dissect along the brachiocephalic trunk and follow the
right common carotid branch as it progresses superiorly along the right side of
the trachea to approximately the level alongside the thyroid gland.
(Figure221) (Netter087)
(Netter199)
(Photo7114)
The carotid arteries are encased in a thin tube-like sheath of fascia. Within the carotid sheath are the carotid arteries, internal jugular vein, vagus nerve and some associated deep cervical lymph nodes. Thus, you may need to slit/separate the fascia as you follow the right common carotid along the side of the trachea.
Recall that the left common carotid is a direct branch from the arch of the aorta while the right common carotid is formed by the bifurcation of the brachiocephalic trunk into the right common carotid and right subclavian arteries.
Anterolateral to the sheath is a delicate nerve loop called the ansa cervicalis formed by branches of C1-3. Branches from this nerve loop innervate most of the muscles in the muscular triangle of the neck. Cut through these as needed.
21. Dissect along the lateral side of the brachiocephalic
trunk to isolate the bifurcation of the right subclavian artery and beginning of
the artery course.
(Figure221) (Netter087)
(Netter199)
(Photo7115)
The angle of the artery is slightly posterior as it heads lateral over the first rib towards the arm. You may need to retract the brachiocephalic artery to the left to expose the bifurcation and observe the beginning of the right subclavian artery.
22. Retract the sternohyoid muscle form its normal position
slightly medially so you can approach the right common carotid artery at the
region lateral to the sternohyoid muscle.
(Netter039)
(Photo7116)
23. Continue to follow the right common carotid superiorly
for several inches to expose other sheath contents for the
next steps.
(Netter039)
(Netter083)
The common carotid artery bifurcates into the internal and external carotid arteries at approximately the level of the superior edge of the thyroid cartilage close to the hyoid bone, thus this is typically too high in the neck to be observed at this time. In some individuals with an early bifurcation you may observe that junction. (Photo7117)
Higher in the neck, the external carotid gives rise to a series of branches. We will not be dissecting those in this lab, however the major anteriorly directed branches are:
Superior thyroid artery - This artery along with the inferior thyroid artery supplies blood to the thyroid gland.
Lingual artery - This artery enters the base of the tongue to supply the floor of the mouth and tongue.
Facial artery - This artery passes over the mandible to supply the superficial face below the level of the eyeballs with blood.
24. Dissect laterally and slightly posterior to the common
carotid artery to isolate the right vagus nerve.
(Netter039)
(Netter083)
(Photo7118)
The vagus nerve lies between the carotid artery and internal jugular vein and slightly posterior to them. You may need to retract the vessels to see the vagus nerve.
The nerve continues into the thoracic cavity where it will give rise to the right recurrent laryngeal nerve. We will not be dissecting to that branch.
25. Continue to dissect lateral to the common carotid
artery and isolate the third component of the carotid sheath, the internal
jugular vein.
(Netter039)
(Netter083)
(Photo7118) (Photo7119)
26. Move to the left side of the neck and move the
sternohyoid muscle back into position allowing access to the left carotid sheath
just lateral to the sternohyoid muscle.
(Netter039)
(Photo7120)
27. Dissect open the left carotid sheath to expose the left
common carotid artery, left vagus nerve, and left internal jugular vein.
(Netter039)
(Netter083)
(Photo7121)
(Photo7122)
The common carotid artery bifurcates into the internal and external carotid artery. This bifurcation occurs too high in the neck for us to observe to this point, occurring approximately at the level of the hyoid bone.
PROCEDURE - Root of Neck
28. The following steps are to be performed only on the left side of the donor.
29. On the left side only, transect the sternohyoid muscle
as close to the sternal attachment as possible and reflect the muscle
superiorly.
(Figure749b)
(Netter035)
(Photo7123)
30. Insert a blunt probe or instrument under the
sternothyroid muscle and transect the muscle as close as possible to the
sternum.
(Figure750b) (Netter035)
(Photo7124)
31. Reflect the left sternohyoid and sternothyroid muscles
superiorly exposing the left lobe of the thyroid gland.
(Netter035)
(Photo7125)
32. Using a Stryker saw, cut through the left clavicle
approximately one third of the distance from the sternum to acromion (i.e. 2-3
inches from the sternal end).
(Figure786) (Netter035)
(Photo7126)
33. Continue the Stryker cut deeper through the segment of
the first rib underneath the clavicular incision.
(Figure786) (Netter194)
(Netter195) (Photo7127)
34. Grasp the excised segment of bone and cut through
residual soft tissue connections so you can remove the excised section of
clavicle, manubrium, and 1st rib.
(Figure786) (Netter194)
(Netter195)
(Photo7128)
(Photo7129)
35. Reposition the cut end of the left brachiocephalic vein
and observe that it crosses over the trachea and left common carotid artery then
bifurcates.
(Figure221) (Netter210)
(Photo7130)
The left brachiocephalic vein bifurcates to give rise to the left internal jugular vein and left subclavian veins. This bifurcation is typically just lateral to the left internal carotid artery.
The vein may have been transected as you removed soft tissue to excise the clavicle segment above. If that is the case, observe just the cut end.
36. Reflect the left brachiocephalic vein and remove fascia
to expose the left common carotid artery from the origin at the arch of the
aorta to the carotid bifurcation.
(Figure221) (Netter210)
(Photo7131)
37. Isolate the left vagus nerve and follow the nerve
inferiorly as is courses posterolateral to the left common carotid and posterior
to the left subclavian vein before it crosses anterolateral over the arch of the
aorta.
(Figure223) (Netter210)
(Netter213)
(Photo7132)
You may see cardiac splanchnic nerves crossing the aorta just anterior to the left vagus nerve.
Cardiac splanchnic nerves can be present as a single nerve bundle or present as a series of small nerve fibers nerves hidden in fascia depending on the individual. Thus, these nerves may not be visible in every donor.
38. Retract the left vagus nerve and dissect through the
fascia surrounding the left subclavian artery to expose the initial branches
from this vessel.
(Figure754a) (Netter240)
(Photo7133)
The first part of the subclavian artery we can observe in this region (lateral to the anterior scalene muscle) has three branches. Typically, at this stage of dissection we will only observe the vertebral artery which is the first branch from the subclavian artery.
Vertebral artery: The first and largest branch coursing superiorly. The vertebral artery will course through the transverse foramina of the cervical vertebra to enter the skull and supply the posterior brain with blood.
Thyrocervical trunk: This trunk emerges from the subclavian artery on the superior side and almost immediately splits into additional branches. One of these will be the inferior thyroid artery and the others cross to supply neck and shoulder. We will not dissect for this vessel.
Internal thoracic artery: The internal thoracic artery arises just where the subclavian artery crosses the first rib. The artery emerges on the anteroinferior side of the subclavian artery and runs inferiorly on the inside of the chest plate. Since this artery was transected during removal of the chest plate only a short stub may be present with most of the artery on the chestplate.
39. Follow the left subclavian artery laterally and observe
that the artery is more posterior to the vein.
(Figure754a) (Netter037) (Netter040)
(Photo7134)
The subclavian artery passes posterior to muscle fibers of the anterior scalene muscle, while the subclavian vein passes anterior to the muscle.
This is an important clinical arrangement, as the subclavian vein positioned anteriorly can be readily entered with a needle using the clavicle as a landmark.
The separation from the subclavian artery by the anterior scalene muscle minimizes the likelihood of a needle entering the artery by mistake.
The phrenic nerve travels from C3,4,5 along the anterior surface of the anterior scalene muscle to enter the thorax.
40. When your study is complete, remove the wooden block from under the donor and return it to the foot of the shelf below your table.
Post-Lab Daily Clinical Review Cases
Each lab has several multiple choice practice cases to reinforce understanding of the material within the lab and associated lectures. These are optional to review at home for consolidating and testing understanding.
CHECKLIST
Skeletal Structures
Hyoid bone
Thyroid cartilage
Cricoid cartilage
Soft Structures
Sternocleidomastoid muscle
Omohyoid muscle
Superior belly
Inferior belly
Strap muscles
Sternohyoid muscle
Sternothyroid muscle
Thyrohyoid muscle
Common carotid artery
Subclavian artery
Vertebral artery
Thyrocervical trunk
Internal thoracic artery
Subclavian vein
Internal jugular vein
Brachiocephalic vein
Brachiocephalic trunk
Vagus nerve
Phrenic nerve
Thyroid gland
Left and right lobes
Isthmus
{kind=link}