Clinical Exercise: Intraosseous Cannulation (Tibia)
Scenario:
An unconscious patient in their late teens is flown into the Shock Trauma facility suffering thoracic and pelvic injury from an unsecured impact during a motor vehicle collision. The patient is exhibiting rapid blood pressure drop during the helicopter evacuation and is experiencing difficulty breathing from the thoracic injury.
The airway members of the trauma team immediately start working around the patient to manage the acute respiratory distress. The emergency medical technicians on the medevac helicopter report they were having difficulty inserting an intravenous line during transport and could not deliver fluids into the circulation.
Diagnosis:
The major torso injuries coupled with rapid blood pressure loss indicates significant vascular trauma and risk of exsanguination (bleeding to death) from as yet unidentified internal rupture of a vessel or vessels. The hypotensive emergency (blood pressure drop) coupled with the report of difficulty in intravenous insertion from the EMT's, makes you suspect there is significant circulatory vessel collapse.
You recognize that you need to act immediately to provide a large bolus (volume) of fluid to sustain blood pressure/circulation and you are not confident of being able to establish intravenous access with the suspected vascular collapse. Thus, you need an alternate location to deliver rapid, large boluses of fluid to stabilize the patient at a location that will not interfere with the cardiopulmonary management.
You decide that the best approach is to insert an intraosseous cannula into the tibia so that you can deliver fluid support.
Mechanism:
In cases of vascular collapse it can be difficult (or impossible in infants and young children) to establish a peripheral intravenous catheter. An alternative method is to provide fluid into the marrow cavity of one of the large bones. This marrow cavity of large bones is highly vascularized with drainage into a central venous canal, emissary veins leaving the bone, and onto the central circulation. The marrow cavity essentially functions as a non-collapsible venous access route that can support rapid infusions of large volumes of fluid.
In cases of vascular collapse the intraosseous cannulation procedure is much faster to perform than central or peripheral lines. The method was traditionally recommended only in children (and almost always used in children younger than 6), but studies in the last 15 years have shown that this is an effect approach at all ages. However, in older individuals the thicker bone and smaller marrow cavity can make the approach more difficult and potentially fracture bone in the area.
The proximal tibia is a common site as it provides a flat bone surface, readily palpable landmarks, and only a thin layer of overlying tissue. Other sites in the adult include the distal tibia, proximal humerus, and sternum (supports the highest flow rate, but in our scenario involving cardiopulmonary resuscitation and possible thoracic surgery it would not be usable).
Treatment (perform these steps on the donor in a mock-procedure):
To treat this patient you need to insert a needle through the outer cortical bone layer of the tibia into the marrow chamber. A variety of devices have been developed for this function ranging from needles with flanges/knobs through to motorized drill devices (reducing fracture risk over manual approaches).
PREPARATION: Send a member of your team to the instrument supply tables to fetch two 6-10ml syringes (so someone can work on left and right side of your donor at the same time) and two 16 gauge needles (one per side of the donor). While not the standard intraosseous needle style it will be suitable for the exercise.
CAUTION: exercise care when handling needles to prevent impaling yourself or a colleague. Needle-stick injury is the leading cause of accidental blood-borne pathogen infection in hospital staff.
To view the intraosseous cannulation procedure performed on a
donor:
Intraosseous Cannulation (Tibia) ---
Video
---
Setup:
1) The patient is positioned supine with the knee flexed slightly.
Place a wood block behind the knee to flex and support the joint during the procedure.
2) If time permits the area would be cleaned with antiseptic and a local anesthetic injected.
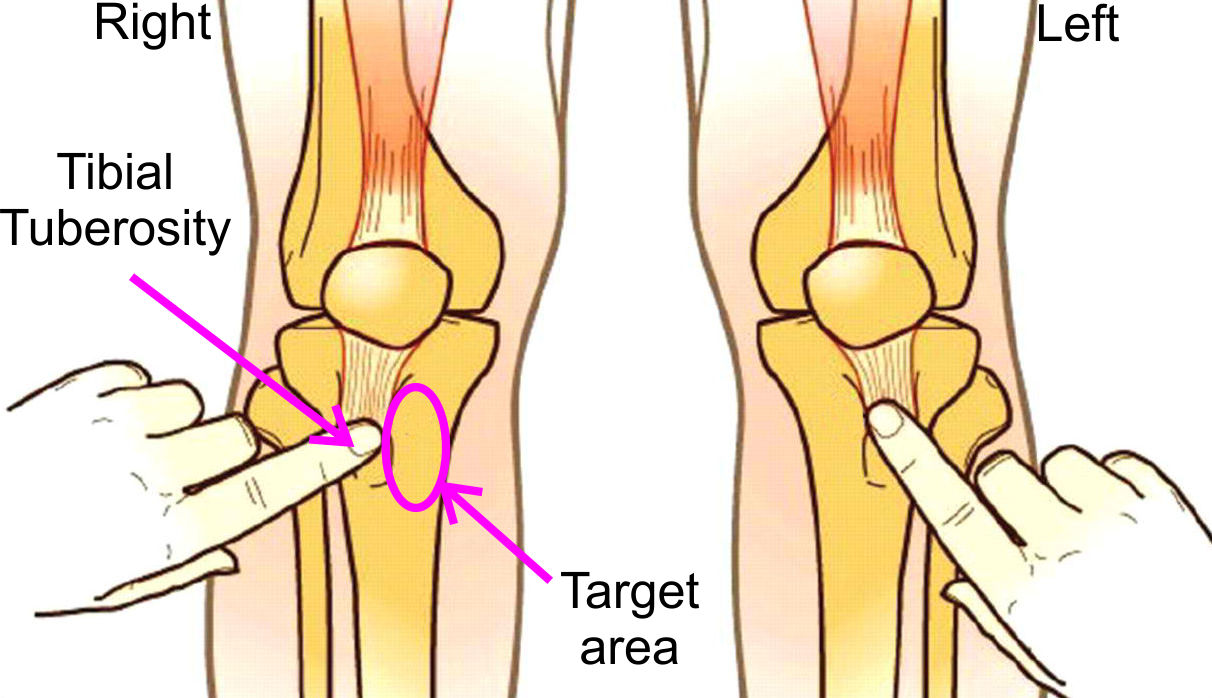
3) Identify the tibial tuberosity slightly inferior to the knee joint by palpation.
This is the 'bump' of bone to which the patella tendon inserts.
4) Palpate for the flat area of the tibia slightly medial to the tibial tuberosity (either or both legs can be used).
5) Angle the needle approximately 10-30 degrees from perpendicular directly inferiorly and insert the needle through subcutaneous tissue aiming at the flat tibial bone target area.
6) Upon reaching bone, hold the needle tightly and press the point of the needle against the bone while rotating the needle with a back-forth twisting motion.
Firm (but not forceful) pressure should be used. Excessive pressure could result in bone fracturing in an elderly patient. It will take anywhere from 5 to 15 back-forth twists to penetrate depending on the stature of the individual. A larger individual with thicker cortical bone may require more twisting back-forth cycles.
The twisting motion rotates the tip of the needle and, in a manner similar to a trepanning drill bit, the tip of the needle will cut a channel through the cortical bone into the marrow chamber.
7) Continue the press/twisting until there is a popping sensation and drop in the pushing resistance, indicating that you have entered the marrow chamber.
8) At this step in a patient you would connect a gravity IV line and begin fluid delivery. Faster rates of infusion can be achieved by manual infusing of 30-60ml fluid boluses.
You can try injecting 10-20ml of wetting agent through the needle with your syringe. Hold the needle base with a hemostat and remove (untwist) the syringe so you can fill it with some fluid. You may find that blood clotting within the venous spaces of the marrow cavity limit how much fluid you can infuse in a donor tibia.
There should be enough space on the tibial surfaces for everyone to have a chance to perform an intraosseous cannulation. Use a new/fresh needle for each insertion as the process of perforating the bone will blunt each needle.
NOTE: when finished the procedure ensure that the syringe and attached needle
are collected in one of your trays and transported to the sharps containers for
disposal.
Do not attempt to re-cap a needle - Re-capping is a leading
cause of needle-stick injury.
Never transport needles by hand - Always transport entire
syringe/needles in a tray.
Outcome:
The rapid infusion of fluids stabilizes the blood pressure allowing the trauma surgery team to determine the extent of the patient's injury. After considerable trauma surgery the patient makes a full recover, and hopefully recognizes the importance of wearing a seatbelt in a motor vehicle.